Haemostasis – Background
Hemostasis is a collective term used to describe the body’s defence mechanism to prevent blood loss and finally dissolve the clot all via combination of multiple complex physiological process coming together. This fine balance of haemorrhage and thrombosis is termed as hemostasis and any imbalance in either or both can a fatal to patient’s life. The reasons for any imbalance in normal hemostasis could by “Provoked” like a Major surgery or an active cancer or liver disease but most reasons are Unprovoked (Hereditary).
Need for Haemostasis testing:
To understand the underlying reasons for the defects in hemostasis that could cause bleeding or thrombosis, a sequential workup is required backed with quality coagulation (Hemostasis) reports for prognosis, prophylaxis and management of patient’s health. Almost all specialities in medical profession need quality results in coagulation, thus clinicians frequently order coagulation tests for their patients for general health understanding to pre-operative and post-operative decisions.
The science behind haemostasis testing
Thrombosis and hemostasis testing is the IN-VITRO study of the ability of the blood to form clots and to break clots IN-VIVO. As thrombotic and hemostasis pathways form a part of critical disease state ranging from haemophilia to strokes and heart attacks, the testing of patient’s capabilities in thrombosis and hemostasis is a critical diagnostic tool. Should a patient’s ability to form clots in-vitro fall outside of the established norm or should certain markers be out of the normal range, the plasma sample is further assayed to determine the reason for the problem. These assays are in standard use in all hospital laboratories. The coagulation analyser’s primary usefulness is to remove the selectiveness in determining the exact second a clot forms in a sample in-vitro.
Coagulometers
Coagulometers (automated coagulation instruments) used in clinical laboratories have become increasingly complex, and the evaluation of such instruments is complicated and time consuming. The criteria in selecting a coagulation system for a laboratory that is large, processing more samples per day for both routine to speciality assays could be very different vis a vis a medium to small size lab where flow of samples per day are quiet predictable and low. Irrespective of the size of the laboratory the general guidelines for a clinical laboratory while selecting a right coagulation system could be derived from instruments assessment of safety, carryover, precision, bias, linearity, testing capabilities and correlation. Choosing a right vendor is also a significant criterion.
POCT Devices
Unlike the coagulation devices used in the lab that uses plasma as the sample, the POCT devices use whole blood. The POC devices are not a perfect product for laboratory use however they are really handy and often reliable when it comes to home use cases for patients on OAT (oral anticoagulation therapy) to monitor their INR values with a simple finger prick drop of blood being applied on a cartridge and results being read on the POC device within minutes. There also are professional use case models extending the parameters from the regular PT INR to APTT, FIB and TT on a simple whole blood. The qLabs from Micropoint marketed in India by Operon biotech is a perfect example of both personal POC device and as well as professional use POC
Current trends in automated coagulometers:
Coagulation analysers are now marketed as a “system” or “package” and include a set of recommended reagents, tailored for that particular instrument is now in commonplace. Consequently, the evaluation of coagulometers alone has become increasingly difficult and also irrelevant to the situation in most routine laboratories as its always the combination of Instrument and reagent system. These are marketed as a package and not just as stand alone with flexible ownership and buyback/upgrade options.
Current trends in semi-automated coagulometers:
Unlike the automated coagulation analysers which are mostly sorted, structured and packaged along with well-defined reagents/controls/consumables and offered in flexible ownership options including reagent rental, partial rental schemes, part payment basis the semi-automated systems are largely open type. The semi-automated systems are available as stand-alone for purchases with no clear mandate or binding on reagent use. User opts for best available reagent and consumable brands suitable for his lab ranging from small pack reagents to liquid stable. Internal quality control use among semi-automated users is a rare thing to find. There also is a lack of subject knowledge among these user group and clear absence of standardisations is a general finding. Tests barely go beyond PT and aPTT in this kind of setup.
Levels of Coagulation Automation
| Level | Description | Examples |
|---|---|---|
| The testing includes manual operations and the measurements are visual. While the temperature is maintained by water bath or heat block the end point is determined visually by the technician. Timer is initiated and stopped also by the technician. | Tilt Tube method | |
| Semiautomated | The testing includes manual operations and the measurements are automated. The semi auto device maintains the temperature on its own and the technician manually dispenses the sample/reagent at appropriate times after which the instrument reads the end point and displays the results | Fibritimer Zeta -1 Fibritimer Zeta – 2 |
| Automated | All reagents and samples are automatically pipetted by the analyzer instrument. Analyzer contains monitoring devices and internal mechanism to maintain and monitor constant 37° C temperature throughout testing sequence. Timers are initiated and clot formation is detected automatically. | Operon XL – 1000 C Operon XL-1000e |
MECHANICAL METHOD
Mechanical measurement methods depend on the detection of the physical formation of fibrin strands that stops a moving mechanical device that ultimately either completes or opens an electrical circuit.
Any test that has fibrin formation as its end point can be determined using the Mechanical Method. The Zeta-1 uses Custom made unique design cuvette with curvy-linear path at the base and a stainless-steel ball inside the cuvette.
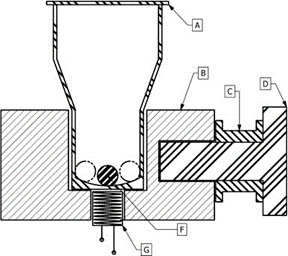
A periodic magnetic field imparts a sustained pendular motion along a curvilinear path to the stainless-steel ball within the inner perimeter at the bottom portion of the cuvette.
The ball deflects on the curvilinear path, moving each time Left and Right in the track in a pendular motion. The ball movement is continuously monitored. The instrument registers any change in the ball’s movement caused due to change in turbidity/viscosity of the test solution and reads it as a fibrin clot. The results are generally displayed in Seconds.
At the start of coagulation, the fibrin filaments will impede the movement of the ball. thereby changing the deflection frequency of the ball’s movement. A sensor registers these changes, automatically stopping the time measurement when the ball ceases to move completely.
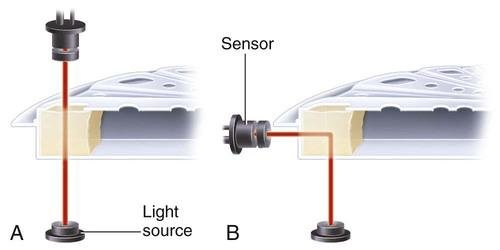
Photo-optical (turbidometric)
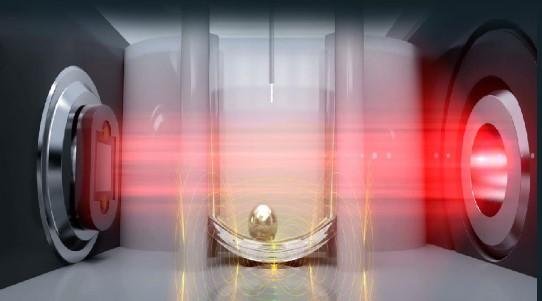
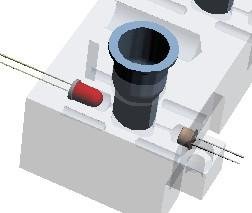
Optical method is LED assisted focusing of the light on the “test solution” wherein the desired wave length is beamed and on the other side the light passed through the “test solution” is captured through the optical receivers. Basic setup is as shown below.Effectively the amount of light received by optical receivers is not the same as the incident light and that change is indicative of the current coagulation state of the “test solution”.
Below is the graph depicting TIME Vs ABSORBANCE CHANGE
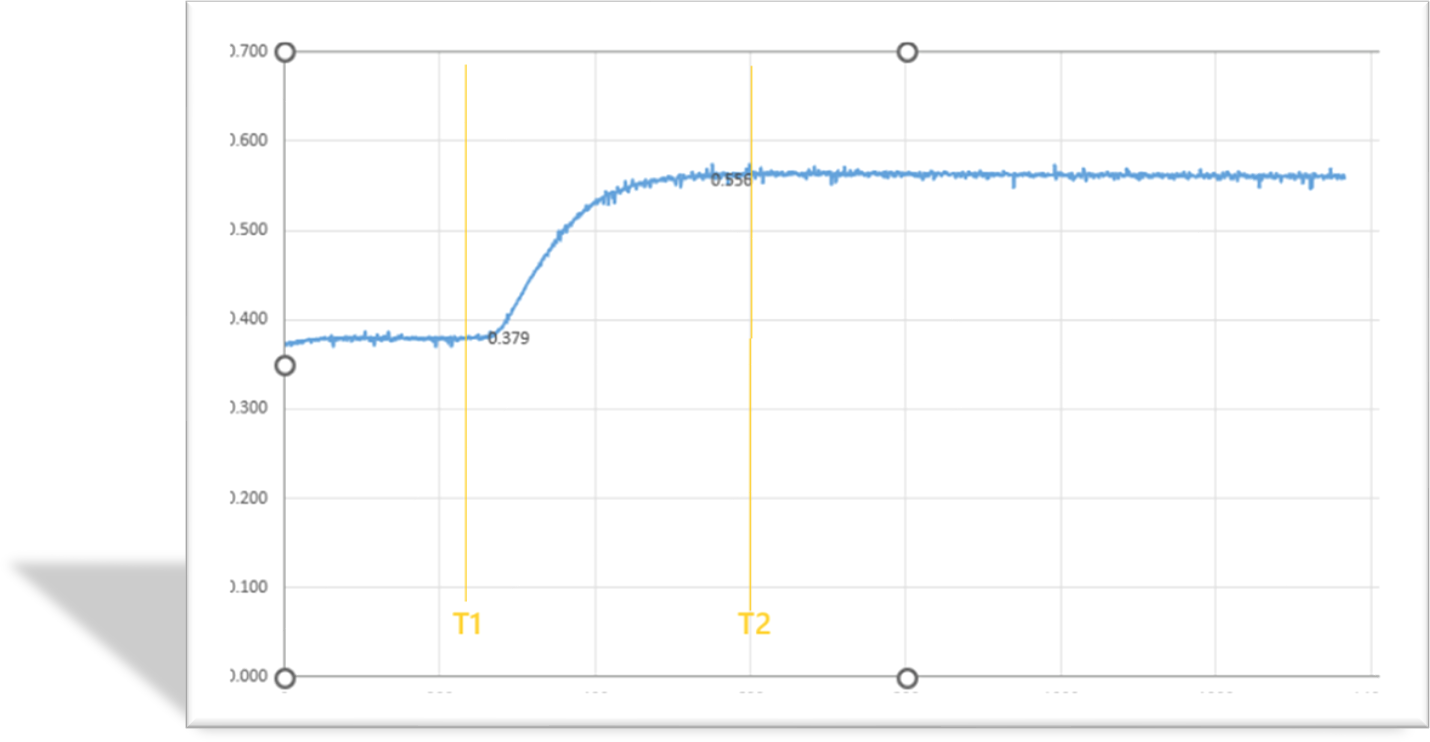
As expected, the intensity of light received at the optical receiver is decreased based on the chemical reaction/turbidity developed and instrument reads the final value.
This phenomenon is used to find the rate at which the intensity decreases.
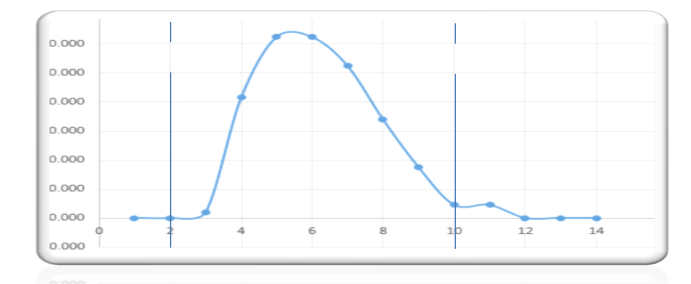
The algorithm in the microcontroller determines the slope and finds out the “bell curve” as represented above. With this, the left point of the bell curve and right point of the bell curve are determined – with 70% of the maximum slope. Average of this left (T1) and right (T2) values are calculated and that would indicate the coagulation time
• Nephelometric
Nephelometry is a modification of photo-optical end-point detection in which 90-degree or forward-angle scatter, rather than OD, is measured. A light-emitting diode produces incident light at approximately 600 nm and a photodetector detects variations in light scatter at 90 degrees (side scatter) and at near 180 degrees (forward-angle scatter). As fibrin polymers form, side scatter and forward-angle scatter rise (Figure 47-3).4,5 The timer stops when scatter reaches a predetermined intensity, and the interval is recorded.
• Chromogenic (amidolytic)
Chromogenic (synthetic, amidolytic) methodology employs a colourless synthetic oligopeptide substrate conjugated to a chromophore, usually para-nitroaniline (pNA). Chromogenic analysis is a means for measuring specific antigen activity. The oligopeptide is a series of amino acids whose sequence matches the natural substrate of the protease being measured.7 Protease cleaves the chromogenic substrate at the site binding the oligopeptide to the pNA, freeing the pNA. Free pNA is yellow; the OD of the solution is proportional to protease activity and is measured by a photodetector at 405 nm. In some instances, a fluorescent conjugate is used; this method is called fluorogenic.
Immunologic
Immunologic assays are the newest assays available in coagulation laboratories and are based on antigen-antibody reactions similar to those used in nephelometry as described previously. Latex microparticles are coated with antibodies directed against the selected analyte (antigen). Monochromatic light passes through the suspension of latex microparticles. When the wavelength is greater than the diameter of the particles, only a small amount of light is absorbed.8 When the coated latex microparticles come into contact with their antigen, however, the antigen attaches to the antibody and forms “bridges,” which causes the particles to agglutinate. As the diameter of the agglutinates increases to the wavelength of the monochromatic light beam, light is absorbed. The increase in light absorbance is proportional to the size of the agglutinates, which in turn is proportional to the antigen level.
Final thoughts
The introduction of new coagulation methodologies has improved testing capabilities and in expanding the test menu. in the coagulation laboratory. There still is a need for further advancements wherein platelet studies, whole blood coagulation studies also if could be merged alongside the conventional plasma coagulation testing thus bringing a better understanding on defects related to hemostasis. While the systems and process are getting more and more automated and getting smarter by the day… the diminishing knowledge and failing acumen among the users on the fundamentals of testing, procedures, results interpretation is a big big cause of worry. As long the systems are functioning the results seem to be in safe hands of technology and once something goes wrong with the technology of systems and automated processes that’s where the danger zone is.
Advances in Coagulometry
Significant advances have been made in the capability and flexibility of coagulation instrumentation. Instruments previously required manual pipetting, recording, and calculation of results, which necessitated significant operator expertise, intervention, and time. Current technology allows a “walkaway” environment in which, after specimens and reagents are loaded and the AI – assisted testing sequence is initiated making the whole testing and reporting easy and seamless.
References: oncohema key, Dacie&Lewis, National Insititute of Health
Questions/ Feedback? We’d love to hear from you! Feel free to write to us on info@operonbiotech.com or comment in the section below.
Disclaimer : This content may be copyright protected. Reproduction, modification, or use without prior written permission is prohibited.